Resource Centre
Discover a wealth of knowledge and insights from the experts at StarFish Medical. Our Resource Centre offers product development tips, reviews of new and cutting-edge technologies, and in-depth articles on regulatory updates and compliance in medical device development.
-

Nigel Syrotuck breaks down REACH SVHC compliance for teams working with material suppliers and compliance questionnaires.
-

We examine when computational modelling and simulation, or CM&S, genuinely supports medical device simulation strategy and when it becomes a costly detour.
-
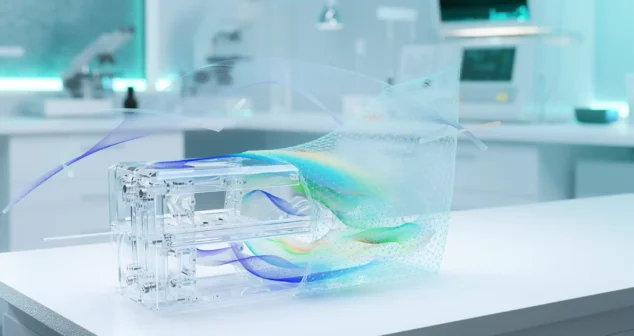
Many teams still underuse CM&S, often bringing it late in device validation, when key decisions have already been made. That approach leaves much of the value of CM&S untapped.
-
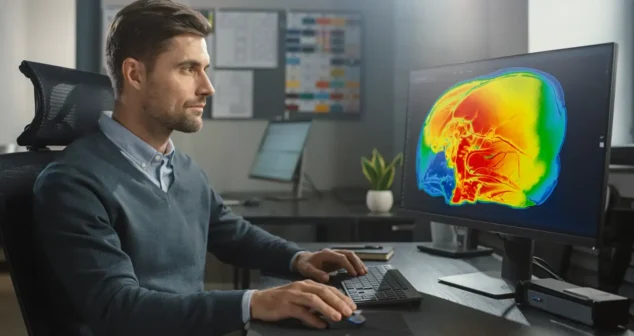
This article traces the Pennes bioheat equation from its 1948 origins to modern multiscale approaches, explaining how engineers select the right level of modelling complexity across device categories.
-

Five methods for building accurate project estimates, from gut feel to bottom-up, plus three add-ons that sharpen any estimate.
-
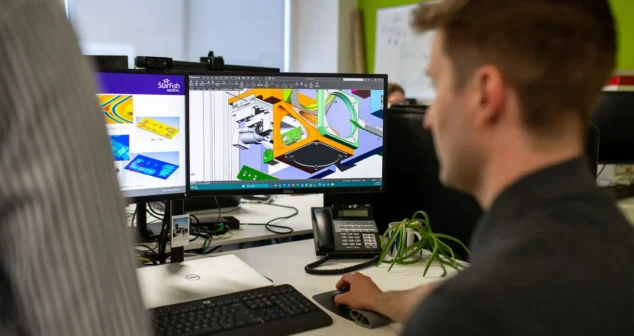
Designers and engineers today have no shortage of tools to improve designs, accelerate timelines, and meet cost targets. The challenge is knowing what to use and when.
-
Nick and Nigel break down what actually goes into the cost of getting a sterilized device into a user's hands, and why up to 30% of costs can sit in places most teams don't plan for.
-

Theranostics combines diagnosis and therapy into a single targeting system, using one ligand to attach to two different radioactive payloads, one for imaging and one for treatment. It represents a significant shift in how cancer is being identified and treated. But the theranostics delivery workflow tells a different story.
-
Most medical devices were designed for clinical settings, not the patients and caregivers who increasingly rely on them at home. Here's what good home-use device design actually requires.