
US Reimbursement Codes for Medical Devices
TL;DR
FDA clearance opens the door to market, but it does not guarantee a device will be adopted or paid for:
- Reimbursement in the US operates through three interdependent pillars — coding, coverage, and payment — each governed by different rules depending on whether a device is used in an inpatient, outpatient, or physician office setting.
- Medicare and private payers evaluate new devices against clinical and economic evidence; without an identifiable advantage over the existing standard of care, payers are unlikely to invest the time to establish coverage.
- Companies should develop a reimbursement strategy in parallel with their regulatory strategy, identifying applicable existing codes or pursuing new ones early, since the absence of the correct code can block payment entirely.
A Primer on the US Reimbursement System for Medical Devices
The main success criteria for medical device companies after earning FDA regulatory clearance is securing positive coverage decisions from payers. While regulatory approval is sufficient to get a product to market, it has no bearing on product adoption. The availability of reimbursement has a direct impact on therapy adoption – it can “make or break” a product1. This primer provides an overview of US reimbursement codes and when they are used to help determine coverage and payment for medical devices.
Please note that the information provided is at an introductory level. Always consult a reimbursement strategy expert for device specific code analysis.
Why is reimbursement as important as regulatory?
Often medical device companies underestimate the barriers associated with securing payer coverage. If providers are not paid adequately, they will be reluctant to offer a new therapy, negatively impacting the market potential. Companies need to research the delivery chain for their products and develop an integrated reimbursement strategy that identifies a path to clinical adoption and broad payer coverage.
The US healthcare system involves multiple government and private payers – the reimbursement processes differ by payer type. The most important players in coverage decisions are Medicare (which accounts for 21 percent of national healthcare expenditure) and large commercial insurers.
Reimbursement describes how commercial insurance plans (or the government) pay for items or services provided by medical professionals. It can be broken down into three major components: coding, coverage and payment (see Fig. 1).
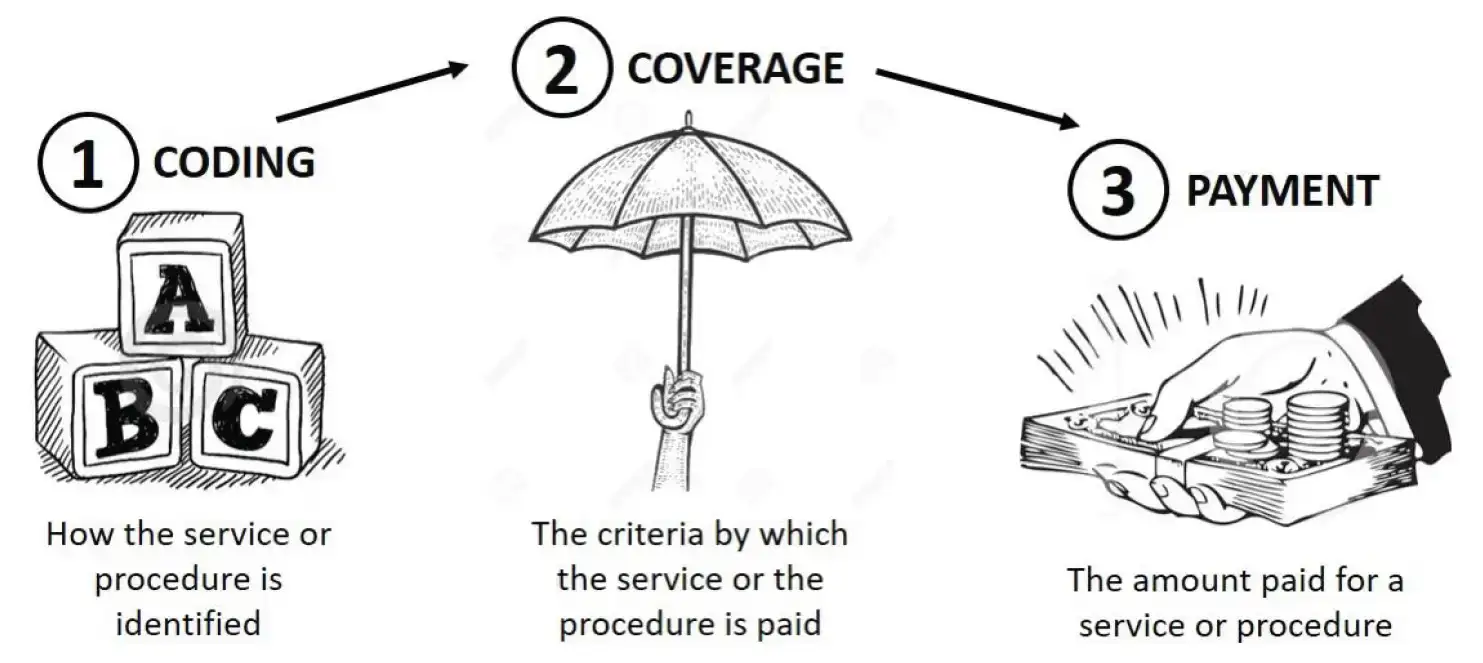
Figure 1. The three pillars of reimbursement for medical devices.
In the US, physicians and healthcare facilities are billed and paid separately. A portion of procedures is often paid directly by those receiving the treatment. Physicians bill for the procedures they perform at different rates depending on whether the procedure is performed in a facility setting (e.g. hospital) or a non-facility setting (e.g. office or clinic). Physician rates for work performed in facilities are generally lower than physician rates for work performed in non-facility settings, because the facility provides support and infrastructure for the procedure which is billed separately2.
Medical device companies need to understand how their device may or may not fit within current payment methodologies and become fluent in the language of medical billing (i.e. the various medical coding systems). This chain of events is shown in Fig. 1 in reverse order, starting with payment.
Payment – aka ‘Show Me the Money’
Payment is the transfer of money from the payer to the provider for the provision of health care services. Payment amounts for procedures or medical devices do not depend on the price tag a manufacturer sets for their product, but rather reflect its perceived clinical value. These payment amounts can be fixed or based on usage costs.
Payment mechanisms will vary by setting (e.g. hospital, ambulatory surgery setting, or physician’s office) and may be paid separately or packaged (bundled). Several providers may be paid separately for the same service. For example, a procedure performed in a hospital; the hospital, the surgeon, and a radiologist could all receive separate payments3. Depending on the setting in which the device is used, different coverage criteria will apply, different codes will be reported, and different payment rates will be assigned.
No Money Yet?
Companies could consider working with specific payers and providers on pilot programs to establish the clinical or economic benefits of their devices4. Alternatively, the product may have to be on cash (patient pay) basis until a compelling case for coverage can be made.
Coverage – Payers’ Willingness to Reimburse for a Certain Procedure/Device
Coverage refers to a payer’s decision to provide program benefits for a specific product or service. Coverage decisions typically include assessment of whether or not technologies are “reasonable and necessary” or meet respective payer medical necessity criteria. Limited coverage for technology or procedure often leads to minimal market uptake while broader coverage allows for an optimal market uptake. Medicare and private payers institute coverage criteria to ensure appropriate utilization of products and services and to control costs.
Create a team to do a ‘What If’ analysis. What if I do more? What if I do less? What if I don’t do anything ‘x’? This helps determine the critical steps and will highlight any potential consequences.
1) Medicare
Medicare is the largest single-payer in the US and plays a significant role in setting reimbursement for medical devices. Medicare is a national program, but coverage decisions are made by the local Medicare Administrative Contractors, thereby yielding coverage decisions that vary across the US.
Medicare includes national or local coverage policies:
A) National Coverage Determination (NCD)
The NCD process consists of three steps: initiation, review and completion. Formal requests for an NCD can be initiated either by:
- An outside party who identifies an item or service as a potential benefit (or to prevent potential harm) to Medicare beneficiaries
- Or by internal agency personnel
Once received, Medicare will make a benefit category determination. The item is then listed with pending coverage issues on the Medicare website until a final determination is made.
B) Local Coverage Determination (LCD)
Medicare contractors develop LCDs when no NCD exists, or when further clarification of an NCD is needed. LCDs can be established with the intent to create a payment policy or manage utilization. Some contractors have quotas on establishing a certain number of LCDs. NCDs will pre-empt LCDs only when a final NCD is issued and local contractors must then amend or withdraw any inconsistent LCDs.
In Medicare, beneficiaries may request a “quality of care review” and question the level or kind of services provided by their practitioner or provider. Complaints triggering review can be about the quality of medical care, including concerns about the receipt of poor or inadequate treatment from health care workers, incorrect or inadequate medication, inappropriate or failed surgeries and procedures, or premature discharge from a hospital. Medicare is looking to improve the quality of health care and control costs by changing the way they pay for health care – paying doctors, hospitals, and other providers more for high-quality care, and less for poor quality care. This approach is often called pay-for-performance or value-based purchasing and is also being used by private payers5.
2) Private Payers
Private payers cover all Americans receiving health insurance through their insurers. Private payers have payer-specific coverage, payment and technology assessment processes. Medical devices are covered under the medical benefit and, for the case of private payers, new and emerging devices are reviewed by the Technology Assessment committee within each organization to determine if they are eligible.
A Health Technology Assessment (HTA) is utilized by the Technology Assessment committee as a decision-making strategy that compares the effectiveness and cost of new technology with competing existing technologies (see Fig. 2). HTA platforms evaluate the costs, effectiveness, and broader impact of health care solutions for those who plan, provide, or receive care, taking into account clinical, social, humanistic, economic, legal, and ethical issues6. Payers rely heavily on HTA when making coverage determinations.
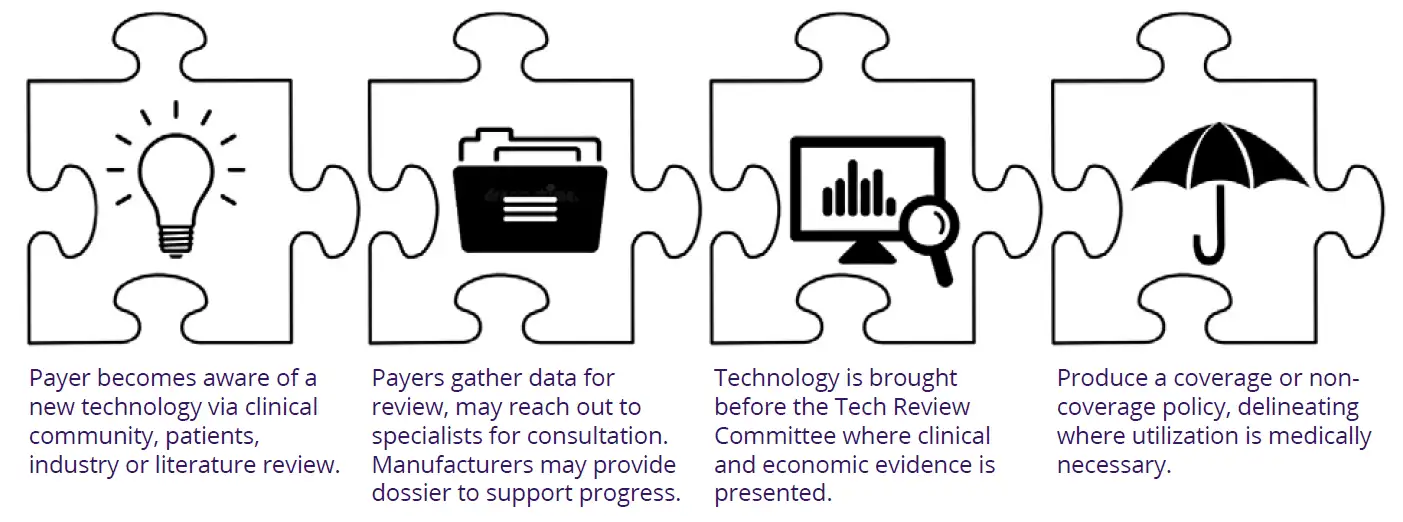
Figure 2. Overview of the Health Technology Assessment (HTA) process for new technology.
3) Self-Pay
Many procedures are not covered by insurers (e.g. elective cosmetic surgery or LASIK eye surgery, etc.) and patients must pay out of pocket. However, it has been found that some procedures (e.g. MRI), while being covered by insurance, are often less expensive if patients choose to pay cash up front and not submit claims through insurance7. These inconsistencies in coverage are a very hot topic in the US healthcare system, and the current caveat is buyer beware.
New Devices Must Prove Clinical or Economic Advantage to Earn Payer Attention
Cost-effectiveness studies can be helpful when a new technology can deliver non-inferior results less expensively or when results are superior, but the costs are higher. If the costs are comparable to the existing standard of care, the new device needs to be demonstrably better8. Payers often will not invest the time to analyze new devices that cannot identify a clinical or economic advantage.
Coding – Learning the ABCs for Inpatient and Outpatient Procedures
Coding provides a standard mechanism for payers and providers to identify diagnoses, medical services, procedures, drugs, devices, laboratory tests, and supplies (see Table 1). Standard alphanumeric symbols are used to identify the procedure/device to facilitate smooth communication between payers and healthcare providers. Coding is the link between coverage and payment.
The Current Procedural Terminology (CPT) (also known as the Health Care Financing Administration’s Common Procedure Coding System (HCPCS) Level I) procedure code tells the payer what service was performed and also (in most cases) determines the amount of payment. The International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) diagnosis code, on the other hand, tells the payer why the service was performed. If the diagnosis code does not meet the payer’s criteria for medical necessity, all payment for the service will be denied.
Medical coding involves extracting billable information from the medical record and clinical documentation, while medical billing uses those codes to create insurance claims and bills for patients. The types of codes used vary by provider and by location of service. The following is a brief guide to codes and reimbursement-related classifications used by hospitals for inpatient and outpatient admissions.
| Code | What It Stands For | What It Is | How It Is Used for Reimbursement | Who Manages the System |
|---|---|---|---|---|
| APC | Ambulatory Payment Classification | Describes hospital outpatient services1 | Medicare sets a specific, uniform amount that all hospitals will be paid for the same outpatient services | Maintained by the Centers for Medicare and Medicaid Services (CMS) |
| CPT (HCPCS I) | Current Procedural Terminology; aka HCPCS Level I codes (under the Health Care Financing Administration’s Common Procedure Coding System) | Describes medical, surgical, and diagnostic procedures (but not diagnoses themselves); can be performed in a clinic, inpatient hospital, or outpatient hospital setting | Medicare makes physician reimbursement decisions, but not for covering facility-related reimbursement2 | Maintained by the American Medical Association (AMA) on behalf of the CMS |
| HCPCS Level II | Health Care Financing Administration’s Common Procedure Coding System – Level II | Describes supplies and services obtained outside the physician office that are not covered by a CPT code3 | Hospitals/Non-hospitals/ Non-physician supplier used to submit claims. Medicare makes reimbursement decisions for procedures, services, equipment, and supplies utilized in an outpatient setting, but not typically billed by physicians | Maintained by the CMS. HCPCS II may apply to supplies used as part of a procedure, but may not be separately reimbursable beyond APC |
| ICD-10-CM | International Classification of Diseases, 10th Revision, Clinical Modification | Classifies patient diagnoses and mortality data from death certificates | International standard from which US clinical modifications are derived and used in the reimbursement process | Managed by the CMS and the National Center for Health Statistics (NCHS) in collaboration with the World Health Organization (WHO) |
| ICD-10-PCS | International Classification of Diseases, 10th Revision, Procedure Coding System | Classifies morbidity data and describes procedures associated with utilization of health services in the US | Physicians use to justify the CPT and/or DRG codes they use to bill for a particular patient encounter; also used by public and private payers for auditing the use of healthcare codes by providers | Same as above |
| MS-DRG (DRG) | Medicare Severity – Diagnosis Related Group | Describes procedures and other services performed in a hospital setting | Medicare makes non-physician related reimbursement decisions for procedures performed in an inpatient hospital setting | Maintained by the CMS |
- APC – includes diagnostic procedures, cancer therapies, ambulatory surgery, clinic and ER visits, partial psychiatric hospitalization and surgical pathology
- CPT – does not include codes needed to report and cover medical items or services billed by suppliers other than physicians
- HCPCS II – includes durable medical equipment, prosthetics, and orthotics
APC Codes
The Ambulatory Payment Classification (APC) is a system used for the billed CPTs group to determine the outpatient payment(s). Procedures performed in physician office extensions or procedure centers that are not certified Ambulatory Surgery Centers (ASCs) are reimbursed based on the Medicare Physician Fee Schedule.
Medicare uses comprehensive APCs (C-APCs) which bundle certain procedures with all related ancillary services which are commonly provided/performed in conjunction with a primary procedure (e.g. imaging services). If a CPT code maps to a C-APC, there is only a single payment for the procedure and the associated ancillary services.
Medicare takes an average of six months to create claims reimbursement codes for medical devices, and temporary technology add-on codes that are designed to reduce the financial burden on providers still leave large gaps between reimbursement and device costs.
CPT and HCPCS Procedure Codes
Procedure codes complement diagnosis codes by indicating what providers did during an encounter. The two main procedure coding systems are the Current Procedural Terminology (CPT) codes and the Healthcare Common Procedure Coding System (HCPCS). Many HCPCS and CPT codes overlap, but HCPCS codes can describe non-physician services, such as ambulance rides, durable medical equipment use, and prescription drug use. CPT codes do not indicate the type of items used during an encounter.
In an outpatient setting, hospitals bill CPT codes on a “per procedure” basis. Unlike the inpatient setting, ICD-10 codes do not directly impact payment for outpatient procedures. Hospitals can potentially receive multiple payments for individual patients when several services and procedures are performed in an outpatient setting.
Here is a quick overview of how to look up a CPT code using the free CPT Lookup Tool*:
- Go to the American Medical Association (AMA) website and ‘Create an Account’
- Review the ‘End-User License Agreement’ and click ‘Agree’; this will bring up the Search page
- Search page; choose a state and city OR
- If the CPT code is already known, to see what it means; input the 5-digit CPT code and ‘Submit’; (the Search Results page will include the Medicare payment information)
- If the CPT code, is not known but the procedure or service name are known try to find the CPT code using the name(s)
*Note: CPT Lookup Tool is limited to five code lookups per day.
For example, the CPT code 99454 covers remote monitoring of physiological data with a device, and using California as the state:
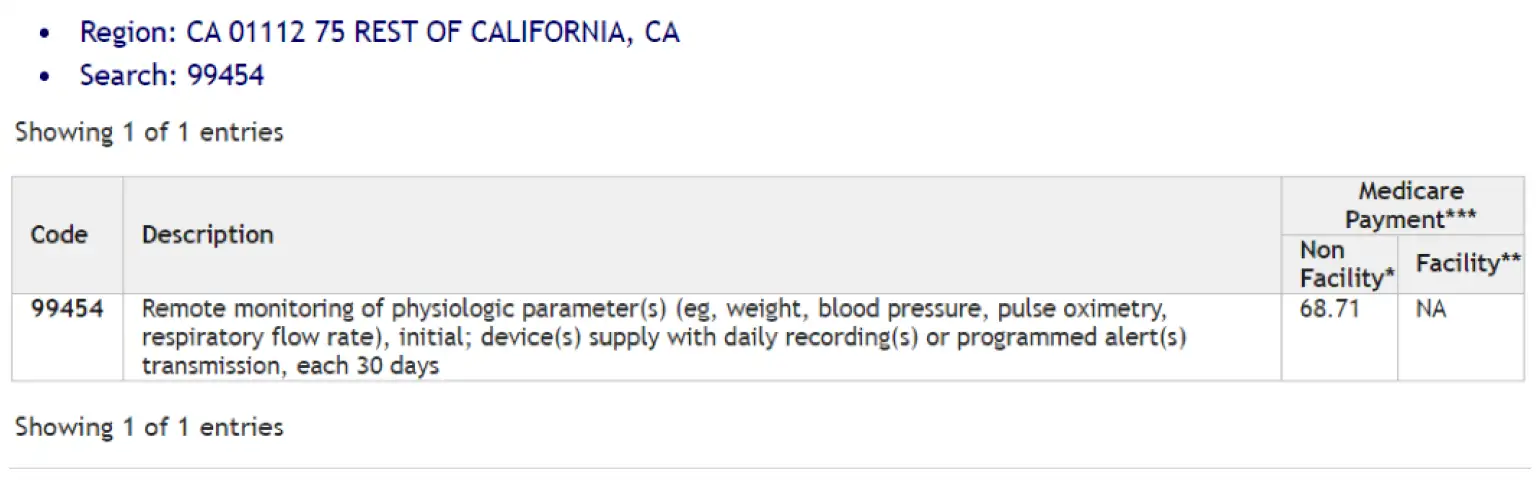
Using the keywords ‘remote’ or ‘monitor’ to search, several other devices came up, but not the previous 99454 CPT code. Searchers may get lucky with search terms if the terms are for a very specific technology or a unique body part, but often that is not the case. It may take several iterations of using various search terms to find the relevant code. There are many subscription-based CPT code databases available online which do allow unlimited CPT code search access for a fee
Outpatient Prospective Payment System
ICD-10 Codes
Diagnosis codes are key to describing a patient’s condition or injury, as well as social determinants of health and other patient characteristics. The International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) is used to capture diagnosis codes for billing purposes. The ICD-10 code set has two components: the ICD-10-CM (clinical modification) codes for diagnostic coding, and the ICD-10-PCS (procedure coding system) for inpatient procedures performed in the hospital.
The ICD-10 codes indicate a patient’s condition or injury, where an injury or symptom is located, and if the visit is related to an initial or subsequent encounter. These codes support medical billing by explaining why a patient sought medical services and the severity of their condition or injury.
Inpatient Prospective Payment System
DRG Codes
Inpatient care is defined as a hospital stay needing two or more midnights of medically necessary hospital care. In this scenario, most hospitals are paid based on a Diagnostic Related Group (DRG) basis. The DRG that is used for the patient is determined by the reason for admission (diagnosis), and in some cases, the procedure performed. Hospitals receive a single payment per hospital admission that is designed to cover all services provided (including device and technology costs) during the admission.
When there is more than one diagnosis or procedure performed, the one that is associated with the highest reimbursement will determine the DRG the patient will be classified under. DRG classification can be based on a primary diagnosis only or the combination of a diagnosis and an associated procedure. Medicare uses Medicare Severity Diagnosis Related Groups (MS-DRG) in which reimbursement levels are adjusted if certain complications / comorbidities or major complications / comorbidities are present at admission.
Where Your Device Is Used Determines How — and Whether — It Gets Paid
Identify the setting where the medical device will be used – there are differing coding, billing and payment systems and scenarios that are dependent on whether the technology is utilized in either an inpatient, outpatient, ASC, or physician office setting.
Using Alternative Codes for Temporary Coverage
In many situations, new technology is billable under existing codes, but the associated payment will not adequately cover costs associated with the technology’s use; consequently, hospitals and providers may be unwilling to adopt it. To overcome this challenge, companies may seek to establish a new billing code that provides higher reimbursement, work with providers to request additional coverage under existing codes, or request temporary pass-through payments.
CMS provides companies with the option of applying for a New Technology Add-On Payment (NTAP) to cover the cost of new medical technologies deployed in the inpatient setting. If approved, CMS pays a marginal cost factor — 50 percent of the cost of the new device or technology, or 50 percent of the overall incremental costs associated with the new technology, in addition to the full DRG payment.
CMS also provides the opportunity for companies to apply for pass-through APC payments for hospital outpatient procedures. These payments are reserved for new, expensive-but-highly-beneficial devices that are used in procedures with existing APC codes. The pass-through typically is calculated as the cost of the device, minus the cost of the device already included in the APC that is being replaced.
Companies can also apply for a category III (temporary) code while they await the issuance of a category CPT I code for their new medical technology or procedure. This provision allows companies to build a history of widespread usage with the AMA that will support the establishment of a CPT I code. However, no set payment fee will be established, and it can take years to transition to a category I code. Furthermore, companies run the risk that their device or procedure will be labelled experimental, potentially disqualifying it from coverage by some payers.
Alternatively, companies can use a miscellaneous CPT code while they wait for a category I code. Miscellaneous codes provide a mechanism for providers to submit claims for a service or item as soon as it is FDA-approved. Miscellaneous codes exist for most organs or body systems (e.g. CPT 38999 – Unlisted procedure, hemic or lymphatic system). When a miscellaneous code is used, the healthcare provider must provide additional documentation justifying the use of the device as part of their attempt to obtain coverage. This typically involves writing a lengthy procedure note describing the patient’s medical condition, the procedure itself, a list of all supplies used, the rationale for using the new procedure or technology, and supporting clinical data9. Payers then decide whether to provide any coverage for the procedure.
Reimbursement Strategy Belongs in Your Development Plan from Day One
A medical device company should start reimbursement planning in parallel to developing the regulatory strategy. A successful reimbursement strategy has two major goals: (1) to demonstrate medical benefit and added value to secure coverage, based on clinical study evidence; and (2) to identify the appropriate existing coding for the new product or recognize the need to create a new or revised code.
Since medical device reimbursement primarily depends on the coding system, the absence of the correct code may prevent payment for a device or service. Working with CPT code consultants and a medical specialty society can help a company obtain new CPT codes to ensure reimbursement for new medical devices, or determine if the new device fits within an existing CPT code.
If new products do not obtain the desired amount of reimbursement or, even worse, are not covered by payers, then physicians and hospitals are highly unlikely to buy and utilize the new products. How the device will be used will heavily influence how it will be reimbursed.
Having a business plan in place that is reflective of how it will be reimbursed gives payers direct insight into the value of the medical device and will help to ensure a successful market launch.
StarFish Medical can assist with planning a regulatory approach that aligns with the marketing and reimbursement strategy. Like three legs of a stool, medical devices need to have all three working together to achieve a successful outcome.
Resources
- Medtech, Look to Marketing for the Solution. White paper. 2019.
- Premier Healthcare Database: Data That Informs and Performs. White paper. 2019.
- Understanding the Medical Billing Process. Radiology Associates of Ridgewood.
- Out of the valley of death. How can entrepreneurs, corporations and investors reinvigorate early-stage medtech innovation? White paper. 2017.
- What Is Pay for Performance in Healthcare? Article. NEJM Catalyst. 2018.
- Health technology assessment and economic evaluation: Is it applicable for the traditional medicine? Article. ScienceDirect. 2021.
- Hospitals and Insurers Didn’t Want you to See These Prices. Here’s Why. Article. NY Times. 2021.
- Why Isn’t Innovation Helping Reduce Health Care Costs? Article. HealthAffairs. 2020.
- Unlisted and Unspecified Procedure Codes. Article. HarvardPilgrim HealthCare. 2021.
Does Your Device Have a Path to Reimbursement?
Your Reimbursement Questions, Answered
What is medical device reimbursement and why does it matter?
Reimbursement describes how government programs and commercial insurers pay for items or services provided by medical professionals. For medical device companies, securing positive coverage decisions from payers is the primary success criterion after FDA clearance, because reimbursement has a direct impact on therapy adoption and market potential.
What are the three pillars of medical device reimbursement?
Reimbursement breaks down into coding (how a procedure or device is identified), coverage (a payer’s decision about whether to pay for it), and payment (the amount transferred from payer to provider). All three must be addressed for a device to achieve broad clinical adoption.
What is the difference between CPT codes, HCPCS codes, and DRG codes?
CPT codes describe medical and surgical procedures and are used across inpatient, outpatient, and clinic settings. HCPCS Level II codes cover supplies and services not captured by CPT codes, such as durable medical equipment. DRG codes apply in inpatient hospital settings and determine a single bundled payment per admission based on the patient’s diagnosis and, in some cases, the procedure performed.
How does Medicare decide whether to cover a new medical device?
Medicare makes coverage decisions through National Coverage Determinations (NCDs), which apply nationwide, or Local Coverage Determinations (LCDs) issued by regional Medicare Administrative Contractors when no NCD exists. Private payers conduct their own Health Technology Assessments, evaluating a device’s clinical and economic evidence before a Technology Assessment committee.
What options do companies have if no reimbursement code exists for their device?
Companies can apply for a New Technology Add-On Payment (NTAP) for inpatient settings or a pass-through APC payment for outpatient procedures. They can also use a temporary category III CPT code or a miscellaneous CPT code while awaiting a permanent category I code, though both options carry risks including delayed timelines and the possibility of being classified as experimental.
When should a medical device company start planning for reimbursement?
Reimbursement planning should begin in parallel with regulatory strategy development. Because coding, coverage, and payment all affect how a device reaches providers, early planning helps companies identify the appropriate codes, build the clinical evidence payers require, and avoid launching a cleared device that providers cannot bill for.
Alexandra (Sandy) Reid is a former QA/RA Specialist at StarFish Medical. She has a PhD in plant molecular biology, has filed several patents on manufacturing therapeutic proteins in plants, and was a reviewer for Canadian Federal natural sciences and engineering grant applications before joining StarFish. She provides support to StarFish clients in the form of documentation generation, review and general quality and regulatory guidance for medical devices.
Images: Adobe Stock & StarFish Medical
Related Resources

Jason McGee explores how the Rightness Trap Medtech dynamic can quietly erode enterprise value in medical device companies.

Scott Phillips, CEO of StarFish Medical, sits down with Peter van der Velden, Managing General Partner at Lumira Ventures, to explore the strategic thinking behind major MedTech transactions and investments.

Every MedTech startup begins with a hypothesis, an idea that could transform patient outcomes, simplify delivery of care, or improve how clinicians diagnose and treat patients.

In Medtech, a successful exit isn’t just about having an innovative device, it’s about building a business that potential buyers and investors can clearly see a future in.