
Sterile Assurance Level Explained
What does a sterile assurance level actually mean, and how do you prove sterilization worked? In this Bio Break episode, Nick and Nigel walk through how terminally sterilized medical devices are verified, what methods are used to sterilize them, and how biological indicators are used to challenge the process in the hardest-to-reach places.
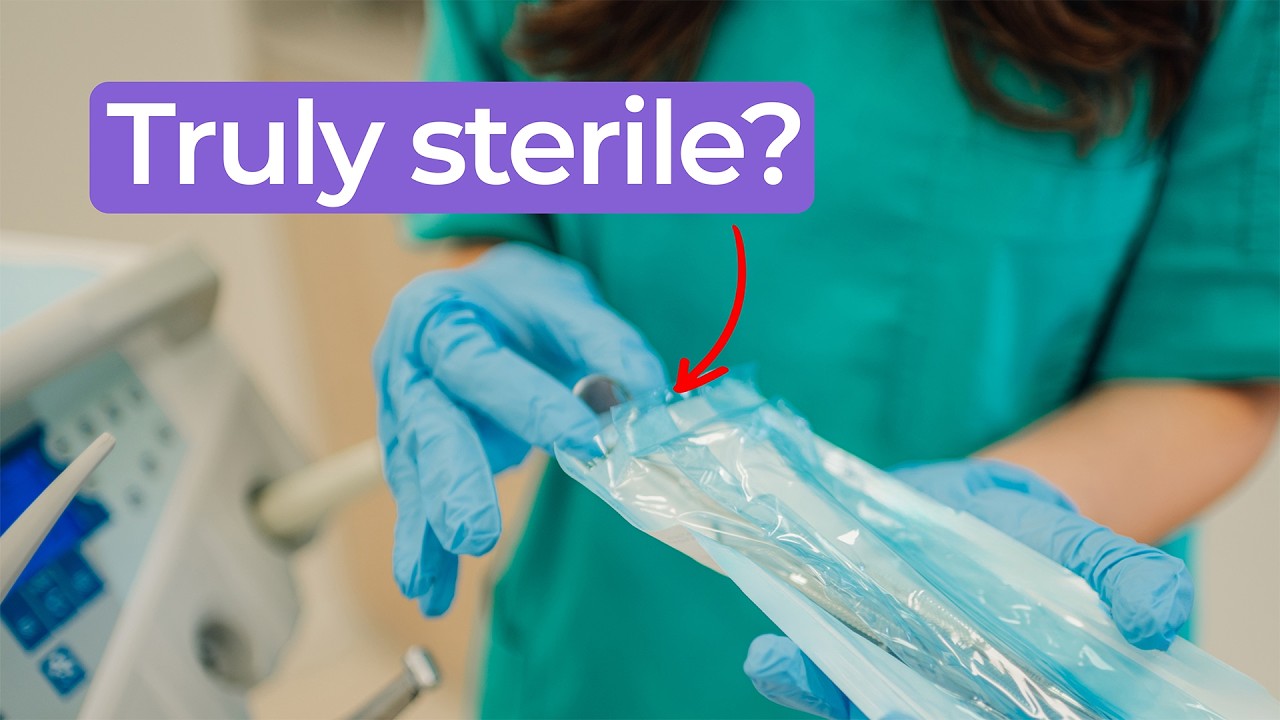
Terminally Sterilized Devices and Common Methods
Many medical devices that cross Nick and Nigel’s desk are sterile disposables. Devices sterilized at the end of their production process are called terminally sterilized. The common accepted sterilization methods are ETO, a gas that permeates through sterile barrier packaging and kills microorganisms throughout the device, and radiation, which includes electron beam, X-ray, and gamma radiation that pass through materials and destroy microorganisms as they go.
Why Device Geometry Creates Sterilization Challenges
Each method has its challenges depending on device geometry. Devices with long lumens, essentially internal tubes, present a particular difficulty. ETO gas has to make its way into the center on its own without being forced in, which takes time and isn’t always straightforward. Radiation can sometimes be better suited for long lumens, though not always. Adapting the sterilization approach to the shape of the device is part of the validation work.
Biological Indicators: Proving the Process Worked
Verifying that sterilization actually reached the most difficult areas is Nigel’s domain as a microbiologist. Biological indicators, which are bacterial spores, are placed in challenging locations such as the center of a long lumen. After sterilization, they are taken to the lab and incubated. If any growth appears, the sterilization didn’t work.
For radiation sterilization, the dose level can also be measured at the point of interest, though getting instruments into tight geometries can be its own challenge. In some cases an analog approach is used, and final product testing for bacterial remnants is another option.
What SAL 6 Actually Means
The target for terminally sterilized devices is sterility assurance level six, or SAL 6. Nick describes this as roughly a one in a million probability that any viable microorganisms remain after sterilization, equivalent to a 99.9999 percent chance that they were all eliminated. That statistical benchmark is the level the team shoots for.
What this episode covers
- What terminally sterilized means and why many disposable medical devices fall into this category
- The two common sterilization methods: ETO gas, which permeates sterile barrier packaging and kills microorganisms throughout the device, and radiation including electron beam, X-ray, and gamma, which pass through materials and destroy microorganisms as they go
- Why device geometry, particularly long lumens, creates challenges for both gas and radiation sterilization methods
- How biological indicators, which are bacterial spores placed in difficult-to-reach locations, are used to verify that sterilization worked, and what it means if growth appears after incubation
- Additional verification approaches including radiation dose measurement, analog methods, and final product testing for bacterial remnants
- Nick’s explanation of SAL 6 as approximately a one in a million probability that viable microorganisms remain, equivalent to a 99.9999 percent elimination rate
Enjoying Bio Break? Sign up to get new episodes sent to your inbox.
Related Resources

Nigel Syrotuck breaks down REACH SVHC compliance for teams working with material suppliers and compliance questionnaires.

We examine when computational modelling and simulation, or CM&S, genuinely supports medical device simulation strategy and when it becomes a costly detour.
Many teams still underuse CM&S, often bringing it late in device validation, when key decisions have already been made. That approach leaves much of the value of CM&S untapped.
This article traces the Pennes bioheat equation from its 1948 origins to modern multiscale approaches, explaining how engineers select the right level of modelling complexity across device categories.