
Lasers in Medical Devices
TL;DR
Lasers have been used in medicine for over 60 years and are now standard across surgery, diagnostics, and therapeutics:
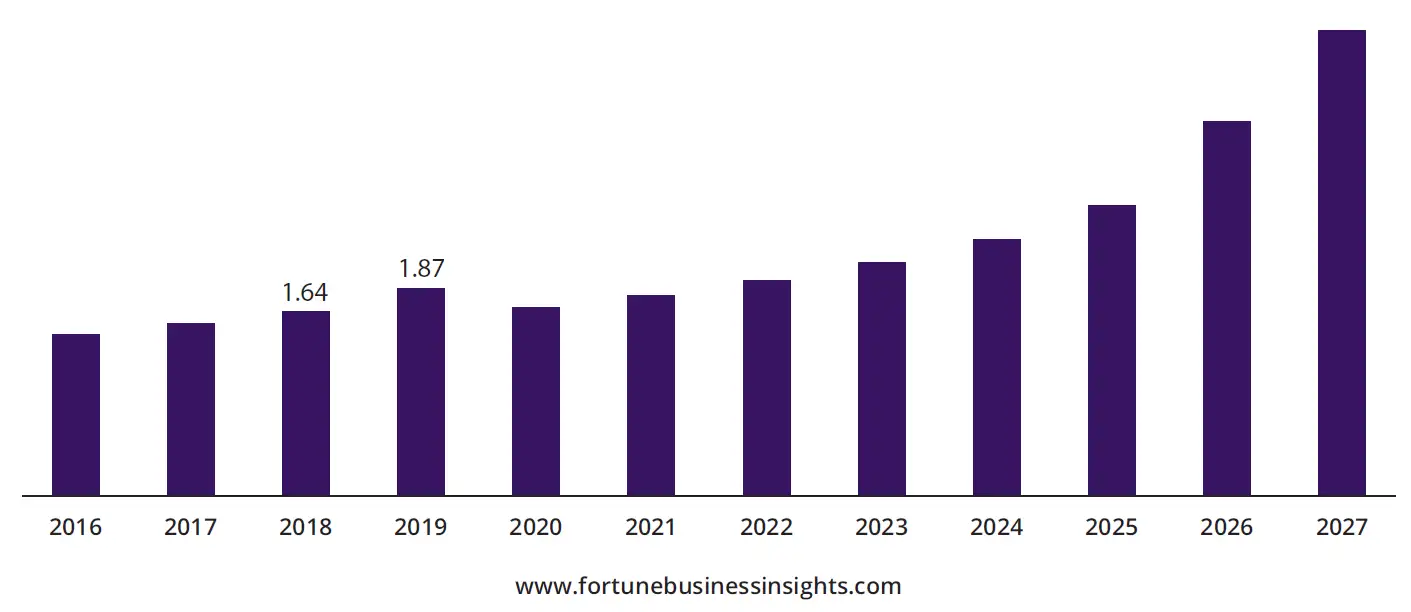
- The North American medical laser market was valued at $1.87 billion in 2019 and is projected to more than double by 2027, reflecting how deeply laser technology has become embedded in clinical practice across dermatology, ophthalmology, urology, oncology, and cardiovascular surgery.
- Laser-tissue interactions fall into four distinct mechanisms — photothermal, photoablative, photochemical, and photomechanical — and selecting the right laser for a medical device depends on matching the mechanism to the intended clinical outcome.
- For medical device developers, lasers should be evaluated wherever they can improve outcomes, reduce equipment costs, shorten recovery times, or lower treatment costs compared to conventional alternatives.
Considering, Choosing, and Implementing Laser-Based Technology for Medical Devices
Over the last six decades, the use of lasers in medicine has grown rapidly. Lasers are now commonly used both as diagnostic tools and in various treatment modalities. This whitepaper is designed for readers considering, choosing, or implementing a laser-based technology in the device they are developing. It discusses the principles of operation of lasers, their useful properties, and their interactions with biological tissues, along with a non-exhaustive overview of the myriad ways in which they have been applied in medicine.
Why Medical Device Developers Should Take Lasers Seriously
Since their inception, lasers have found applications in many medical specialties including dermatology, dentistry, ophthalmology, urology, and oncology, among others [1]. Several unique properties of laser light (directionality, pulsed or continuous output, high peak and/or average powers, and long coherence times/lengths) make it applicable to many different diagnostic and treatment modalities. Laser-based technologies can be a game-changer in medical device development. They should be considered for use in cases where they can improve outcomes, reduce equipment costs, reduce patient recovery times, and/or reduce treatment times/costs.
For the reasons above, the market for medical lasers has continually expanded over the past six decades. The North American medical laser market was estimated to have a value of $1.87 billion USD in 2019, which is expected to more than double by 2027 (even after factoring in the effects of the COVID-19 pandemic) [2]. Lasers are now common in medical practice and will continue to be used for the indefinite future.
North America Medical Laser Market Size, 2016-2027 (USD Billion)
Principles of Laser Operation
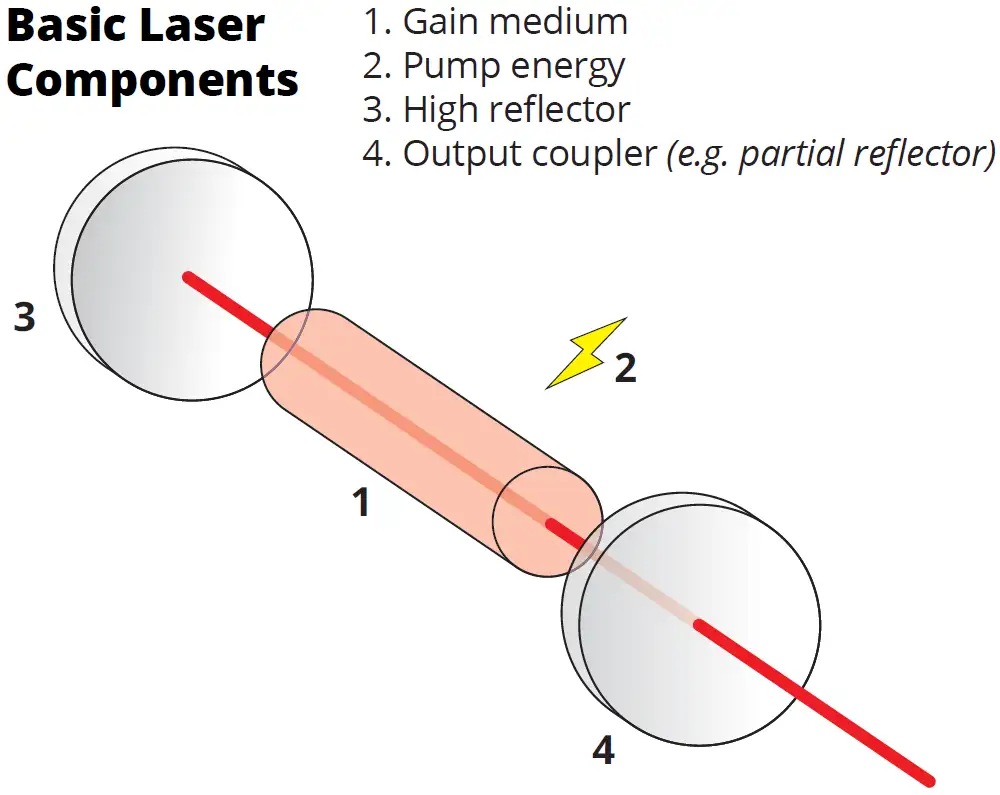
All lasers make use of a physical process called stimulated emission (“laser” is an acronym meaning “Light Amplification by Stimulated Emission of Radiation”). This refers to a process whereby a material in an energized state can be induced to emit photons (light) when light with certain properties is incident on it. Molecules have a discrete number of possible energy “states,” each having a well-defined energy. For stimulated emission to occur, the gap in energy between an excited energy state of a molecule and a lower-energy state must be the same as the energy of the incident photon. In a laser, the molecules in the material undergoing stimulated emission (the “gain medium”) can be placed in a higher energy state by several mechanisms. These include absorption of light from a lamp or a secondary laser (“optical pumping”), passing an electrical current through the medium, or a chemical reaction. When stimulated emission occurs, the emitted photons have essentially the same direction, energy (i.e. frequency/wavelength/colour), and phase i as the incident photons.
A second key element that is present in almost all lasers is feedback produced in an optical cavity (optical feedback). An optical cavity consists of two reflectors between which the gain medium is placed. Most commonly, once the medium is excited, lasing starts first through spontaneous emission whereby photons are emitted from the medium at a certain rate in all directions. Some of these photons reflect from the ends of the cavity, directing them back into the lasing medium. These reflected photons result in stimulated emission, with the additional emitted photons – like the photons that stimulated them – also travelling between the two reflectors of the cavity. The reflection/ amplification process repeats as the light from stimulated emission makes multiple passes through the cavity. Since the emitted photons all have the same phase, direction, and frequency, this process results in an amplified beam with a well-defined direction and frequency. The beam is coupled out of the cavity through various methods – often by using a partially transmissive reflector on one end.
Useful Properties of Laser Beams
Beams of laser light have multiple properties that make them attractive for applications in medicine. These properties include directionality, pulsed or continuous output, high peak and/or average powers, and long coherence times/lengths.
Laser beams are highly directional and can be well collimated (i.e. made to not diverge very much over long distances). This characteristic allows their energy to be directed and confined to a specific location without a lot of residual light elsewhere. Furthermore, well-collimated beams can typically be easily focused down to a very small point. In terms of applications, this ease of focus allows an area affected by the laser beam (such as a location on a surgical site) to be very small and precisely controlled.
Some applications require a laser with a continuous beam (“continuous wave” or “CW” lasers) while others are better served by the application of short pulses of laser light (pulsed lasers). Multiple laser technologies are available in both modalities. Continuous wave lasers tend to be simpler, cheaper, and more robust than pulsed lasers. They can be useful in applications where high average powers are required, or in any technique that requires a continuous source of laser light. Additionally, they typically have a very small frequency bandwidth ii (i.e. they are monochromatic), which can be useful to give high spectral resolution in some applications such as Raman spectroscopy.
Pulses of laser light can currently be made as short as tens of attoseconds (or tens of billions of a billionth of a second) in the most extreme case [3]. Longer pulse durations (femtoseconds to milliseconds) are common in medical laser systems. The physics of short laser pulse generation is somewhat more complex than that of most CW lasers and is outside the scope of this article. In contrast to CW lasers, pulsed lasers have a significant frequency bandwidth (with greater bandwidths being required for shorter pulses iii). Laser pulses can be applied in cases where high peak powers are required, in applications where short pulse durations (or high temporal resolution) are required, and in cases where broad bandwidths are required (such as certain spectroscopic applications).
Lasers can have extremely high peak and/or average powers compared to other light sources, with average powers as high as megawatts, and peak powers as high as terawatts in the most extreme cases. Such extreme peak powers are observed in certain pulsed lasers, as energy is delivered over very short pulse durations. Lasers with high peak power do not necessarily have high average power which also depends on the frequency at which pulses are emitted. As lasers can typically be focused to a very small point, they can have extremely high peak and/or average irradiances (power per unit area) that are sufficient to affect tissue directly or indirectly. In some cases, such as in applications that make use of photothermal effects, long pulse durations (~10-6 to 10-1 seconds) with relatively low peak irradiances (~100 to 106 W/cm2) are used. In other cases, such as in plasma-induced ablation, very short pulses (~10-15 to 10-9 seconds) with very high peak irradiances (~1010 to 1015 W/cm2) are used. The total energy delivered to the treatment area in each pulse is generally comparable in both cases (within a few orders of magnitude). The specific combination of pulse duration and irradiance required depends on the mechanism of action being used [4].
Finally, some laser beams have a long coherence length. This means that there is a well-defined relationship between the locations and timings of the maxima and minima of the laser’s light field. Monochromatic lasers can have very long coherence lengths (up to hundreds of meters). For this reason, they are useful in various interferometric applications which rely on predictable interactions (or “interference”) between waves over long times or distances iv. In contrast, lasers that have a large bandwidth have a short coherence length. This can also be desirable in some applications, though the light source in such cases often does not necessarily have to be a laser.
Laser-Tissue Interactions
There are multiple useful physical mechanisms by which laser light can affect tissue. These are detailed in brief below [4, 5].
Photothermal Effects
Lasers can be used to rapidly heat a volume of tissue. Some of the light energy absorbed by molecules in the tissue is converted to heat through molecular vibrations and collisions. Depending on the laser’s parameters, the rise in heat can be used to affect tissue in various ways. These include coagulation, vaporization and selective thermolysis (heat-induced chemical/cell decomposition).
Photoablation
Lasers can directly induce ablation (removal of tissue) through two mechanisms. The first is through molecular dissociation. In this mechanism, high-energy photons (or multiple lower-energy photons) are absorbed by the tissue’s molecules. The photons have a sufficiently high energy to break molecular bonds, leading to ablation by the immediate dissociation of the molecules.
Second, if a laser is sufficiently intense it can cause a chain reaction that converts the tissue to a ‘soup’ of ions and electrons – a plasma. When initiated with short (picosecond or femtosecond) pulses, plasma-induced ablation has several useful features: minimal thermal damage; the ability to ablate low-absorbing (transparent) tissue; and a reduction in damage to collateral tissues due to the absorption of residual photons by the plasma[4].
Photochemical Reactions
Some chemical reactions are induced by the absorption of photons. Such reactions are called photochemical. In medicine, the primary use of photochemistry is in activating administered drugs called “photosensitizers.” These drugs lead to cell-death of surrounding tissue when light of a particular wavelength is shone on them, inducing a chemical reaction in the photosensitizer and tissue (photodynamic therapy).
Photomechanical Effects or Photodisruption
Intense lasers can induce mechanical effects in tissue. These effects include acoustic shockwaves, bubble formation and cavity formation. While these effects are detrimental in some cases, they have been put to use in breaking up certain tissues, such as kidney or gall stones[4].
Medical Uses of Lasers
The potential of lasers for use in medicine was appreciated very early on in their development. The first example of a laser used in a medical study was reported in 1961 [6], only one year after the development of the first laser. In that experimental study, photocoagulation was demonstrated in an animal retina upon laser irradiation. Two years later in 1963, this approach was experimentally applied to repairing a retinal tear in a human [7]. Concurrently, the first use of a laser in dermatology was demonstrated in 1962 for tattoo removal [8]. Although laser technology has evolved, both of these applications continue to the present day.
In the decades since, the use of lasers in medicine has been continually expanding. Lasers are now standard for several different treatments. Some of the many ways lasers are used in medicine today are detailed below. Given how widespread their use has become, this overview is by no means exhaustive.
Laser Scalpel
One way that lasers are applied generally in medicine is the cutting, vaporizing, or ablating of tissue, as a “laser scalpel”. This technology is often used as a part of conventional surgeries. The scalpel’s laser is delivered to the treatment site either through an optical fiber or via a series of mirrors in an articulating arm. Depending on the application, various types of lasers can be used for this purpose, which typically have the common property that their laser energy is of a wavelength that is absorbed by key molecules in the biological tissue. As of 2017, lasers that use CO2 mixed with other gasses as the lasing medium – or simply “CO2 lasers” – were the most commonly used surgical lasers [9]. Typically, surgical CO2 lasers have relatively high average powers (tens of watts), long pulses (microseconds to hundreds of milliseconds), and may include a CW mode.
Most laser scalpels have the ability to cauterize as they cut, sealing blood and lymphatic vessels. This reduces bleeding during surgery, and reduces post-operative swelling leading to less discomfort and a shortened recovery. However, cauterization of tissue implies there is a small damage zone around the treatment area (which is also true of conventional scalpels). In recent years, lasers that can ablate tissue while leaving virtually no collateral damage have begun to emerge[10]. These lasers do not cauterize surrounding tissues but are useful in applications where limiting the damage zone or reducing scarring is critical.

Figure 1: A Surgical CO2 Laser, the LightScalpel LS-2010.
Ophthalmology
Laser eye surgery is the most common type of surgery for correcting refractive error in vision [11], which is among the most common elective surgeries in the world. Multiple variations exist. LASIK (Laser-Assisted In-Situ Keratomileusis) is perhaps the most well-known. LASIK involves reshaping the cornea by using a computer-guided pulsed laser to precisely remove small amounts of tissue.
Other laser eye surgeries include laser cataract surgery, which is used to replace an opacified lens in the eye with a new intraocular lens. The technique proceeds by making an incision in the cornea, removing the thin capsule in front of the eye’s lens (anterior capsulectomy), fragmenting and aspirating the lens, and finally implanting the new intraocular lens. Although the incision and fragmentation can be done with conventional tools, multiple laser systems have come on the market for this procedure with purported benefits in accuracy and safety. These systems typically output intense but extremely short (femtosecond) pulses and thereby limit the amount of energy that is directed into the eye to complete the surgery.

Laser Vision Correction via LASIK using an Alcon Wavelight EX500.
Lasers also have diagnostic applications in ophthalmology. One example is confocal scanning laser ophthalmoscopy which is used to diagnose macular degeneration and other disorders of the retina. In this technique, a point of laser light is rapidly scanned over the retina vertically and horizontally. Returning light is focused through a pinhole and captured by a photomultiplier tube. A very high-resolution image can then be reconstructed from the collected raster scan. The optics of this technique are such that, in addition to achieving high lateral resolution, images at different depths of the tissue can be obtained with sub-micron depth resolution. It is even possible to combine images at multiple depths to create a 3D image.
Optical coherence tomography (OCT) is an imaging modality that has various uses in medicine, but which is most used in ophthalmology to create images of the retina or the eye’s anterior segment. OCT allows for 3D imaging of these structures with micrometer lateral and axial resolution and allows for imaging of the tissue’s internal structures (in general, scanning laser ophthalmoscopy has superior lateral resolution, but inferior axial resolution, and is not capable of imaging as deeply as OCT).
There are multiple implementations of OCT. In all of them, a beam of bright light is split into two (usually-equal) parts, one of which goes to a reference mirror, with the other going to a sample with the light travelling precisely the same distance between the two. The light in the reference arm is almost completely reflected, whereas light from the sample is reflected in different amounts from different depths in the tissue. Reflected light from the two arms is recombined such that they can interfere while being captured on a detector. By measuring the amount of interference, the reflectivity at a given depth can be inferred. By various means, this measurement is done over a range of depths and lateral positions to create a 3D image of the tissue. The images are similar to those generated by ultrasound, which also measures differential reflections of waves from various depths in tissue, but using acoustic waves rather than electromagnetic ones (i.e. light).
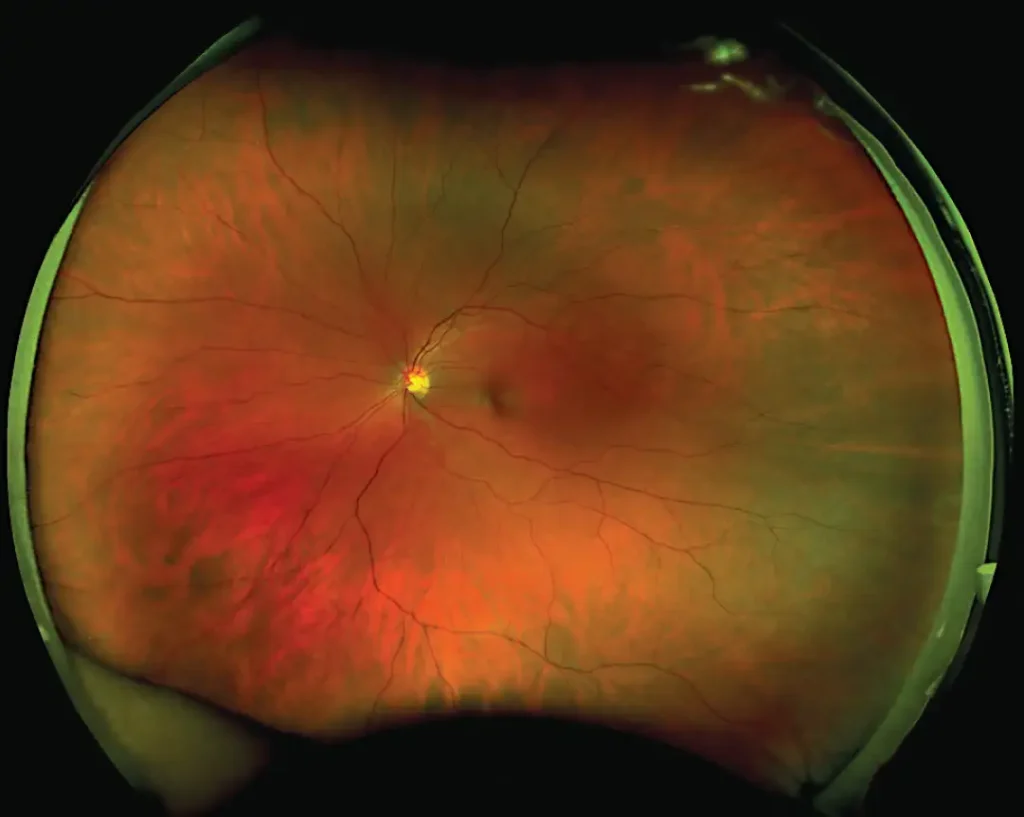
Figure 2: An image of a human retina captured using ultra-wide-field scanning laser ophthalmoscopy. The semi-realistic colors shown are inferred based on scans done with multiple lasers having different colors.
In OCT, a depth scan is performed either by translating the reference mirror or sweeping through a range of wavelengths using a narrowband laser source and capturing the intensity of the interfered light on an intensity detector (time-domain and swept-source OCT, respectively), or by measuring the spectrum of the interfered light with a spectrometer (frequency-domain OCT). By applying mathematical methods to the collected signal, a depth profile (or “A scan”) can be produced, corresponding to the amounts of light reflected at different depths in the tissue. Repeating this process at multiple lateral positions (“B scan”), either by raster scanning or by using appropriate imaging optics, allows for a 3D image of the tissue to be produced.
The type of light source varies between OCT implementations. In time- and frequency-domain OCT, the source must have a short coherence length. This can be achieved with a pulsed laser but is more commonly done using a non-laser broadband light source such as a superluminescent diode. In swept-source OCT, the source is a narrowband laser that is rapidly swept through a range of frequencies. Compared to other implementations, swept-source OCT has been shown to have faster acquisition times, superior image quality, and deeper scan depths [12], though the components required are more expensive at present.
Dentistry
Lasers have many uses in dentistry. They can be applied as a laser scalpel (or “drill”) to ablate both hard and soft oral tissues. Some procedures in which they can be used this way include caries removal, cavity/root canal preparation, gingivectomy/genioplasty, biopsy, lingual frenectomy, and many more [13]. Most types of laser scalpels used in dentistry apply the laser light directly to the tissue under treatment. However, in some cases the laser is used to heat the distal end of the delivery fiber to very high temperatures by placing an absorptive material (such as carbon paper) at the tip. The heat of the tip, rather than the laser light, is then what cuts the tissue [14].
Another application is in the treatment of aphthous ulcers. This is done using low-level laser therapy (LLLT), in which a relatively low-power (<0.5 W) laser is shone on the ulcers over a number of short intervals. Evidence has demonstrated the effectiveness of this procedure [15]. Although the mechanism is poorly understood, the efficacy is believed to be caused by photochemical changes in certain biological molecules.
A common diagnostic test is caries detection using laser-induced fluorescence. It is known that oral bacteria in carious lesions fluoresces when excited by a red laser [16]. This fact can be used to identify caries in the tooth, including ones which may be hidden from visual inspection. One implementation of this method proceeds by shining red laser light into the tooth through an optical fiber and collecting the induced fluorescence through adjacent fibers. The level of fluorescence measured can identify caries with good sensitivity and reproducibility.

Figure 3: The KaVo DIAGNOdent pen. A hand-held device for carries detection using laser-induced fluorescence.
Urology
Benign prostatic hyperplasia (i.e. non-cancerous prostate enlargement) is a common problem among older men. The “gold standard” treatment for this condition is transurethral resection of the prostate (TURP) which involves visualizing the prostate through the urethra and removing tissue. Multiple techniques applying lasers have been used for this purpose [17]. The earliest techniques used neodymium-doped yttrium aluminum garnet (Nd:YAG) lasers, with a wavelength in the infrared of 1064 nm, to induce necrosis in the tissue through heat (interstitial laser coagulation or laser interstitial thermal therapy, LITT). This procedure evolved to use high-power frequency-doubled Nd:YAG lasers, in which the infrared beam is passed through a potassium titanyl phosphate (KTP) crystal, resulting in a green beam at 532 nm. As this wavelength is strongly absorbed by hemoglobin, such a laser is effective at instantly vaporizing the highly-vascularized tissue of the prostate. More recently, the use of Holmium:YAG (Ho:YAG) lasers has come into favor. This laser emits at pulses at 2160 nm, which is readily absorbed by the water in biological tissue. The laser light has a sufficiently high absorption in the prostate for vaporization, and the residual heat is effective in coagulating small blood vessels nearby during the procedure.
The Ho:YAG laser is also particularly effective in the treatment of kidney and gallbladder stones (laser lithotripsy) [17]. In this case, the laser is used in a contact mode in which the fiber tip is placed in direct contact with the stones and fragments them through photothermal effects. Other lasers have been used for lithotripsy, but lacked the ability to fragment every type of stone as the wavelengths emitted absorbed effectively only in dark or colored stones. In contrast, the Ho:YAG laser absorbs in water which is a component of most urinary calculi [18]. For this reason, the Ho: YAG laser is generally preferred.
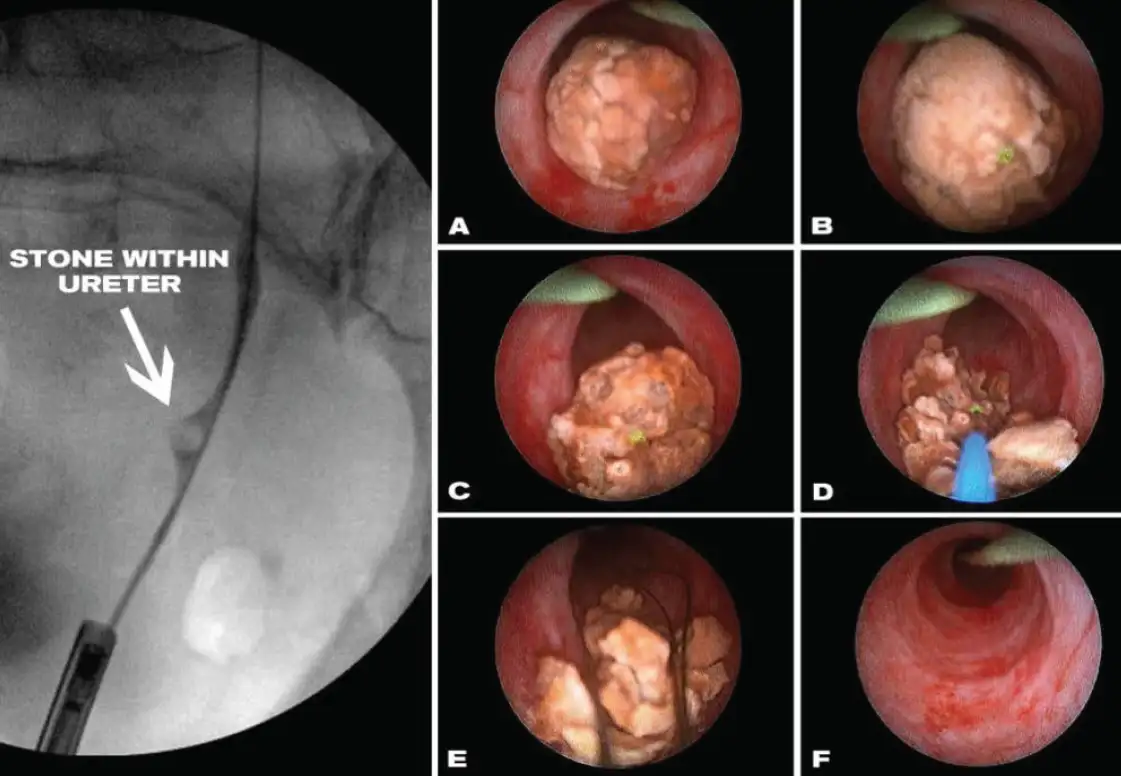
Laser lithotripsy procedure. A) Stone as seen through the scope. B) Preparing to fragment the stone. C/D) Laser fragmenting the stone. E) Removing the stone fragments with basket. F) Cleared ureter.
Oncology
Lasers can play many roles in the treatment and diagnosis of various cancers. They are commonly used to treat superficial cancers that appear on the surface of the body or in the outer layers of internal organs. They have been used to treat cancers or precancers of the colon, lung, skin, esophagus, and brain, among others [19].
Lasers can be used to cut or destroy tumors through direct ablation. LITT has also been used, in which an optical fiber is inserted into a tumor and laser light is used to heat the tumor internally, thus damaging or killing cancer cells.
Another treatment method, as mentioned above, is photodynamic therapy (PDT). In this method, a photosensitizing agent is administered to a patient either topically or through injection. This agent preferentially builds up in cancer cells. When the photosensitizer in diseased tissue is exposed to laser light of an appropriate wavelength, it causes cell death in the tumor through a series of photo-induced chemical processes.
Lasers are also used in a number of methods to diagnose cancer in vivo. This is typically called “optical biopsy” and has the advantages of working in near real-time and not requiring tissue to be excised for examination. Endomicroscopy using confocal laser fluorescence microscopy is one method, which uses laser light passed into the body through a fiber to excite fluorescence in tissue (this fluorescence may be natural or may result from topical or intravenous administration of a fluorophore). The fluoresced light is collected and processed to form a histology-like image that can be used for diagnosis [20]. The optics are such that the tissue is imaged at a certain depth, with fluorescence background emerging from other depths blocked.
Another less common method of optical biopsy uses Raman spectroscopy. In this method, tissue is illuminated with a monochromatic laser and the scattered light is collected in a spectrometer. The scattered light will contain a small amount of light shifted by various frequencies (or equivalently, wavelengths) compared to the incident laser. This is because of inelastic scattering in the tissue, wherein a small amount of energy from the incident photon is transferred to vibrational energy in the tissue’s molecules. The magnitude of shifts in the frequency of the scattered photons is proportional to the energy in the vibrations. Since each type of molecule in the tissue can vibrate only at well-defined energies specific to it (similarly to lasing mediums having discrete energy states), the spectrum of the scattered light provides information about the types and concentrations of molecules in the tissue. While this technique is under investigation for a wide range of cancers, it has yet to reach common clinical use [21].
Cardiovascular Surgery
Various cardiovascular surgeries can be done using lasers. These include laser angioplasty and transmyocardial revascularization [1]. In spite of its utility, cardiovascular laser surgery remains relatively rare throughout the world [22].

The Philips Turbo-Power laser angioplasty catheter. Optimized for the treatment of in-stent restenosis.
Angioplasty refers to procedures used to restore blood flow by opening up obstructed coronary arteries. In laser angioplasty, a laser is guided into the artery and to the blockage through a catheterized fiber. The laser is then used to vaporize the blockage, removing the obstruction. While this technique has some advantages over conventional angioplasty techniques, such as easier passage through chronic or calcified occlusions, the channel opened may be narrow and adjunctive balloon dilation of the artery is sometimes still required.
Transmyocardial revascularization is a procedure used to treat severe angina in patients who cannot undergo a coronary artery bypass graft, or as a supplement to it. In this highly specialized technique, small channels are made through the heart muscle and into the heart’s left ventricle which allows oxygenated blood to perfuse the heart wall. While this procedure does not cure coronary artery disease, it can reduce the symptoms of angina and allow the patient to return to a more active lifestyle. This technique is performed only with a laser (typically CO2 or Ho:YAG) and is the only treatment method for severe angina [1].
Dermatology
Lasers have broad applications in both cosmetic and medical dermatology [19].
As mentioned above, tattoo removal was one of the first applications of a laser used on humans. Laser tattoo removal works by using pulsed lasers to fragment tattoo pigments through photothermal and photomechanical effects induced by the absorption of photons [23]. After fragmentation, the pigments are small enough that they can then be removed by the immune system. In general, the laser used must penetrate sufficiently deeply into the skin to reach the pigment and must have greater absorption in the pigment than in the surrounding tissues. Because of the frequency-dependent absorption of various pigments, different lasers may be required to be effective depending on the tattoo color.
Some other cosmetic uses are hair removal and skin resurfacing [24, 25]. Lasers for hair removal target the melanin in hair follicles, selectively heating basal stem cells leading to reduced hair growth. This procedure is more effective in dark hair that contains more melanin. In skin resurfacing, lasers can be used in either ablative or non-ablative treatments. In the ablative treatment, a thin layer of skin is removed, with the new skin growing in its place appearing younger and tighter. In the non-ablative treatment, the absorbed laser damages aged collagen with heat and stimulates an inflammatory response that leads to the production of new collagen. The non-ablative procedure requires less recovery time than the ablative one but is also less effective.

Laser Tattoo Removal
Vascularized lesions such as port-wine stains and hemangiomas can also be treated with lasers. In these cases, the primary target for laser absorption is hemoglobin. The absorption leads to the selective destruction of the vessels in the highly vascularized tissues through photocoagulation and mechanical injury [26]. Pulsed dye lasers at 585 nm/595 nm are the current standard lasers for this treatment because of their superior efficacy and safety record. However, because these wavelengths have a shallow penetration depth in the dermis, longer-wavelength lasers such as Nd:YAG have been used for the treatment of lesions that go deeper, with variable results.
Lasers Are a Development Opportunity, Not Just a Technology
Lasers have been used in medicine for almost as long as there have been lasers. Their unique properties lead to effective application in many different techniques spanning various medical fields. In the decades since their inception, medical lasers have become more and more commonplace and are now a staple in clinics around the world. Researchers continue to develop new techniques and put them into clinical practice. Lasers have extensive uses in medicine and will continue to be an essential tool for the foreseeable future.
StarFish Medical engineers have over 50 years combined experience in working with cutting-edge laser systems. If you are considering or implementing a laser-based technology in your medical device and seeking additional design or development expertise, please contact us for a free optics consultation.
References
- E. Khalkhal, M. Rezaei-Tavirani, M. Reza Zali and Z. Akbari, “The Evaluation of Laser Application in Surgery: A Review Article,” J Lasers Med Sci, vol. 10, pp. s104-s111, 2019.
- Fortune Business Insights, “Medical Laser Market Size, Share, Growth | Analysis Report,” July 2020. [Online]. Available: https://www.fortunebusinessinsights.com/industry-reports/ medical-lasers-market-101071. [Accessed 1 November 2020].
- T. Gaumnitz, A. Jain, Y. Pertot, M. Huppert, I. Jordan, F. Ardana-Lamas and J. Wörner, “Streaking of 43-attosecond soft-X-ray pulses,” Opt Expr, vol. 25, no. 22, pp. 27506-27518, 2017.
- B. Cox, “Introduction to Laser-Tissue Interactions,” pp. 1-64, 2010.
- H. Lee, “Pulsed Laser-Induced Material Ablation and Its Clinical Applications,” PhD Thesis, University of Texas at Austin, 2003.
- M. Zaret, G. Breinin, H. Schmidt, H. Ripps, I. Siegel and L. Solon, “Ocular Lesions Produced by an Optical Maser (Laser),” Science, vol. 134, no. 3489, pp. 1525-1526, 1961.
- C. Campbell, C. Ritter and C. Koester, “The Optical Laser as a Retinal Coagulator,” Trans Amer Acad Opthal Ontolaryng, vol. 67, pp. 58-67, 1963.
- A. Minivannan, “Basic physics and technology of medical lasers,” Phys. Medica, vol. 32, p. 192, 2016.
- Credence Research, “Surgical Lasers Market Size, Share, Trends, Growth and Forecast to 2026,” 2019. [Online]. Available: https://www.credenceresearch.com/report/surgical-lasers-market. [Accessed 6 10 2020].
- S. Amini-Nik, D. Kraemer, M. Cowan, K. Gunaratne, P. Nadesan, B. Alman and R. J. D. Miller, “Ultrafast Mid-IR Laser Scalpel: Protein Signals of the Fundamental Limits to Minimally Invasive Surgery,” PLoS One, vol. 5, no. 9, p. 13053, 2010.
- Health Canada, “Laser Eye Surgery,” [Online]. Available: https://www.canada.ca/en/health-canada/services/medical-procedures/laser-eye-surgery.html. [Accessed 10 09 2020].
- S. Kishi, “Impact of swept source optical coherence tomography on,” Taiwan J Ophthalmol, vol. 6, pp. 58-68, 2016.
- R. George, “Laser in dentistry – Review,” Int J Clin Dent, vol. 1, no. 1, pp. 13-19, 2009.
- P. Vitruk, “Laser Education, Science and Safety – A review of dental laser education standards,” Dentaltown, June 2017. [Online]. Available: https://www.americanlaserstudyclub.org/ wp-content/uploads/2017/06/laser-education-science-and-safety.pdf. [Accessed 26 November 2020].
- F. Vale, M. Moreira, F. Souza de Almeida and K. Muller Ramalho, “Low-Level Laser Therapy in the Treatment of Recurrent Aphthous Ulcers: A Systematic Review,” Sci World J, vol. 2015, p. 150412, 2015.
- A. Costa, L. Paula and A. Bezerra, “Use of Diagnodent® for Diagnosis of Non-Cavitated Occlusal Dentin Carries,” J Appl Oral Sci, vol. 16, no. 1, pp. 18-23, 2008.
- Ther Adv Urol, vol. 3, no. 2, pp. 81-89, 2011.
- S. Pierre and G. Preminger, “Holomium laser for stone management,” World J Urol, vol. 25, pp. 235-239, 2007.
- B. Azadgoli and R. Baker, “Laser applications in surgery,” Ann Transl Med, vol. 4, no. 23, p. 452, 2016.
- [20] R. Newton, S. Kemp, P. Shah, D. Elson, A. Darzi, K. Shibuya,
- S. Mulgrew and G. Yang, “Progress Toward Optical Biopsy: Bringing the Microscope to the Patient,” Lung, vol. 189, pp. 111-119, 2011.
- I. Santos, E. Barroso, T. Bakker Schut, P. Caspers, C. van Lanchot, D. Choi, M. van der Kamp, R. Smits, R. Doorn,
- R. Verdijk, V. Hegt, J. von der Thüsen, C. van Deurzen, L. Koppert, G. van Leenders, P. Ewing-Graham, H. van Doorn, C. Dirven, M. Busstra, J. Hardillo, A. Sewnaik, I. Hove, H. Mast, D. Monserez, C. Meeuwis, T. Nijsten, E. Wolvius, R. Baatenburg de Jong, G. Puppels and S. Koljenović, “Raman spectroscopy for cancer detection and cancer surgery guidance: translation to the clinics,” Analyst, vol. 142, no. 17, pp. 3025-3047, 2017.
- J. Lin, “Progress of medical lasers: Fundamentals and applications,” Med Devices Diagn Eng, vol. 2, no. 1, pp. 36-41, 2016.
- J. Pozner and D. Goldberg, “Nonablative Laser Resurfacing: State of the Art 2002,” Aesthet Surg J, vol. 22, no. 5, pp. 427-434, 2002.
- E. Azma and M. Razaghi, “Laser Treatment of Oral and Maxillofacial Hemangioma,” J Lasers Med Sci, vol. 9, no. 4, pp. 228-232, 2018.
Considering Laser Technology for Your Medical Device?
Your Laser Technology Questions, Answered
What makes lasers useful in medical devices?
Lasers offer properties that conventional light sources cannot match: high directionality, precise focusability, pulsed or continuous output, and extremely high peak and average powers. These characteristics make them effective for applications ranging from tissue ablation and surgical cutting to diagnostic imaging and photochemical therapy.
What is the difference between continuous wave and pulsed lasers in medical applications?
Continuous wave lasers deliver a steady beam and are well suited to applications requiring high average power or precise spectral resolution. Pulsed lasers deliver energy in short bursts, enabling very high peak powers with minimal thermal damage to surrounding tissue, which is critical in applications like LASIK eye surgery and laser lithotripsy.
How do lasers interact with biological tissue?
Laser-tissue interactions fall into four main categories: photothermal effects, where absorbed light converts to heat; photoablation, where high-energy photons break molecular bonds; photochemical reactions, which activate drugs or biological molecules; and photomechanical effects, which produce shockwaves or cavitation useful for fragmenting kidney stones.
Which medical specialties use lasers most extensively?
Ophthalmology, dermatology, dentistry, urology, and oncology are among the most established fields. Laser eye surgery is one of the most common elective procedures in the world, while Ho:YAG lasers have become the preferred tool for both prostate treatment and kidney stone fragmentation.
What should a medical device developer consider before choosing a laser?
The key considerations are the intended tissue interaction mechanism, the required wavelength and power parameters, whether continuous or pulsed output is needed, and how the laser will be delivered to the treatment site. Regulatory pathway and safety classification should also be addressed early in the development process.
Ryan Field is an Optical Engineer at StarFish Medical in Toronto. His extensive experience in designing, implementing, and operating complex systems combining lasers, optics, electronics and software includes working on medical lasers and surgical microscopes during his post-doctoral studies. Ryan holds a PhD in physics from the University of Toronto, focused on ultrafast laser spectroscopy of molecular spin transitions.
Related Resources
Nick and Nigel breaks down what actually goes into the cost of getting a sterilized device into a user’s hands, and why up to 30% of costs can sit in places most teams don’t plan for.

Theranostics combines diagnosis and therapy into a single targeting system, using one ligand to attach to two different radioactive payloads, one for imaging and one for treatment. It represents a significant shift in how cancer is being identified and treated. But the theranostics delivery workflow tells a different story.

Most medical devices were designed for clinical settings, not the patients and caregivers who increasingly rely on them at home. Here’s what good home-use device design actually requires.

How do you measure comfort in medical device design? Explore the tools, scales, and study design principles that turn a subjective experience into actionable design data.