Resource Centre
Discover a wealth of knowledge and insights from the experts at StarFish Medical. Our Resource Centre offers product development tips, reviews of new and cutting-edge technologies, and in-depth articles on regulatory updates and compliance in medical device development.
-

Medical device teams developing embedded and cross-platform GUIs can accelerate delivery without compromising usability or validation by choosing the right framework early and designing for performance, portability, and maintainability.
-

Compute demands on “the edge”, like embedded sensors or remote devices. have grown significantly as AI has moved from experimentation to deployment. Medical devices are pushing more of their AI functionality onto edge hardware.
-
Medical device cleaning is more complex than it seems. In this Bio Break episode, Nick and Nigel unpack what really goes into cleaning medical devices and why it cannot be treated like a simple wipe-down process.
-
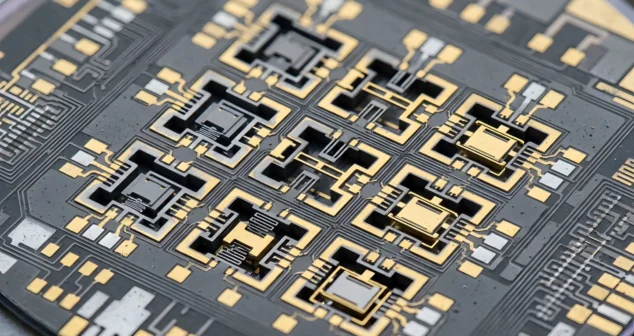
This blog reviews the main families of optical detectors and the major technologies in those families.
-

Jason McGee explores how the Rightness Trap Medtech dynamic can quietly erode enterprise value in medical device companies.
-
Understanding gram positive vs negative bacteria is essential when studying sterility, microbiology, and antibiotic effectiveness. While many people think the difference is only about staining, the reality is much deeper.
-

Nick and Nigel explore the science behind hand sanitizer formulations. They discuss how alcohol interacts with bacterial cells, why water improves its effectiveness, and what the additional ingredients in sanitizer actually do.
-

Scott Phillips, CEO of StarFish Medical, sits down with Peter van der Velden, Managing General Partner at Lumira Ventures, to explore the strategic thinking behind major MedTech transactions and investments.
-

Computer vision technologies such as convolutional neural networks and vision transformers are transforming how AI analyzes medical images, each offering distinct advantages depending on the application and computing environment.