Bioheat Transfer in Living Tissue: History, Models, and Engineering Applications
TL;DR
- The Pennes bioheat equation, introduced in 1948, remains the dominant model in medical device thermal analysis because it is numerically stable, computationally efficient, and widely accepted by regulators.
- More physiologically accurate models (Wulff, Weinbaum-Jiji, non-Fourier) improve realism in specific contexts but rarely change design decisions, because dominant uncertainties typically come from boundary conditions and patient variability rather than microvascular physics.
- Thermal risk modelling applies across device categories: thermal therapies, implantables, wearables, and drug delivery systems each present distinct modelling challenges.
- A tiered approach (baseline Pennes, enhanced Pennes with damage models, targeted complexity) allows engineers to calibrate model fidelity to the decision at hand.
- ASME V&V 40 credibility assessments provide a defensible framework for justifying modelling choices in regulatory submissions.
When heat is generated by medical devices in contact with patients, tissue damage is always a risk. That’s where engineers get involved. Investigative approaches include phantom bench testing and first-principles calculations, but when time-varied results, spatial quantities, or a range of scenarios are needed, computational modelling is the right approach.
Bioheat modelling is critical to understanding thermal risks associated with diverse medical devices, including implants, wearables, radiative treatment modalities, and imaging technologies such as ultrasound and RF. The key is how the body both absorbs and reacts to heat provided by these technologies, and what risk that poses to a patient’s tissue. To understand this in detail it’s worth reviewing the diversity of models developed through the years, and which are best applied to studies.
Blood Flow and Metabolism Change Everything
Classical heat transfer assumes materials are passive: heat diffuses via conduction, convection, and radiation. But biological tissue isn’t passive. It has blood flow, metabolism, and active regulation. These factors fundamentally change how heat moves and accumulates.
A turning point came in 1948 when Harry Pennes introduced what is now known as the Pennes bioheat equation. He added deceptively simple terms to Fourier conduction: a perfusion term that accounts for heat exchange between tissue and blood, and a term for metabolic heat generation. These terms capture that blood carries heat in or out depending on the temperature difference between tissue and arterial blood, alongside baseline metabolic heat generation (e.g., cellular respiration). With that, bioheat modeling became tractable.
Why Pennes Remains the Default Bioheat Model
Pennes’ model makes strong simplifying assumptions: it treats heat exchange as spatially uniform, assumes blood enters tissue at a constant temperature, and models microvascular flow as a volumetric heat sink or source.
These assumptions begin to fail from the effects of large vessels, where directional flow occurs, and through countercurrent heat exchange (cross flow). Even so, Pennes remains the most frequently deployed bioheat model. Why? Because it hits the engineering sweet spot: Pennes is numerically stable, computationally efficient, accurate enough for most applications, and widely accepted by regulators. By default, enterprise commercial modelling tools (ANSYS, Abaqus, COMSOL) all embed it as their default bioheat model.
Where Pennes Falls Short and How Modellers Compensate
There have been many contributions to improve bioheat models over the years, focused on the shortfalls of Pennes and how to address them. Wulff introduced explicit blood flow convection, while Weinbaum-Jiji accounted for countercurrent heat exchange between arteries and veins, improving physiological realism especially in highly vascular tissues like muscle. Non-Fourier models addressed the fact that heat propagation isn’t instantaneous, which is critical for ultrafast heating like laser pulses.
Modern approaches combine, when appropriate, image-derived anatomy, tissue-level bioheat (often still Pennes-based), coupled simulations (e.g., EM, acoustic, fluid), and explicit vessel geometries. These hybrid approaches blend physics across scales: vessel-level details matter for local effects when explicitly modelled, but pressure propagation through tissue from pulsatile flow rarely affects surrounding tissue.
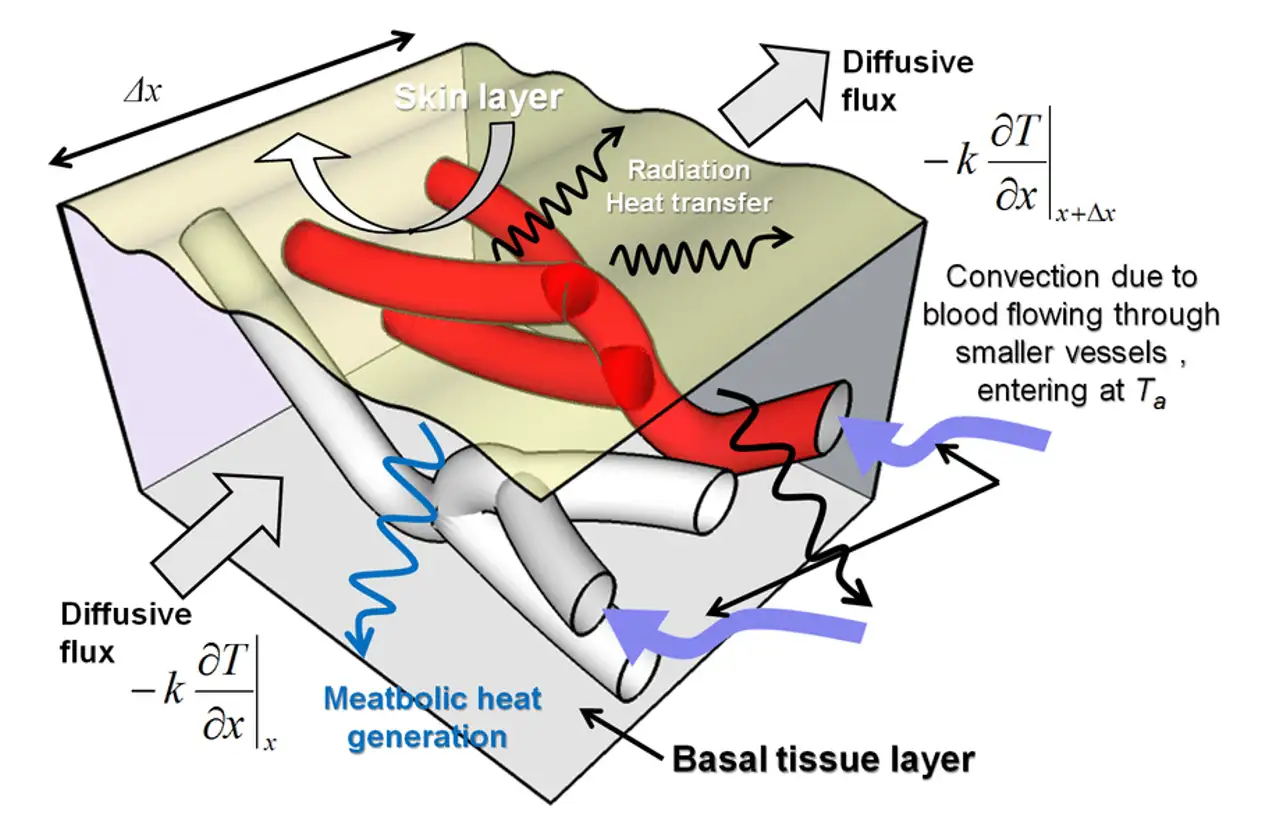
Figure 1 – Pennes Bioheat Domain (source: Alzubaidi et al, Thermography Quantification of Human Perfusion Thermal Signature, Preprints.org, 2018, CC BY 4.0)
More Complex Models Rarely Change the Answer
In theory, these models provide a more accurate picture of tissue reality. In practice, the payoff is heavily context-dependent. They introduce real challenges: parameter uncertainty across perfusion, vessel flow, and tissue properties; high computational cost; difficult validation; and regulatory opacity.
Even when working through these challenges is feasible, the output rarely moves the needle enough to matter. In many cases, device problems have uncertainties dominated by boundary conditions (contact, convection, geometry), device power variability, and patient variability, not those addressed by detailed models such as microvascular heat transfer or arterial effects.
Bioheat Modelling Across Device Categories
Thermal therapies (ablation and hyperthermia). In laser therapies, RF ablation, microwave ablation, and focused ultrasound applications, bioheat modelling can predict a temperature gradient field, lesion size, and tissue thermal dose. One case where Pennes needs augmentation is at higher temperatures (above 50-60°C), where perfusion collapses. A temperature-dependent or damage-dependent perfusion term accounts for this.
Implantable devices. Deep brain stimulators, stents, bone plates, and insulin pumps (the latter subject to heating from absorbed imaging radiation such as MRI) all require bioheat assessment of surrounding tissue temperature rise and compliance with safety limits such as IEC 60601. These are typically low delta-T, steady-state problems, which lend credibility to Pennes with conservative assumptions. Boundary conditions dominate uncertainty, and the higher accuracy from more complex models rarely changes design decisions.
Skin-contact devices and wearables. Monitors (ECG, CGM, BPM), smartwatches, and remote ecosystems for implantables such as pacemakers introduce layered tissue (skin, fat, muscle) and a strong environmental coupling at the boundary. Key challenges include transient heating, contact resistance, and thermoregulation (sweating, vasodilation). Counterintuitively, fat tissue often matters more than perfusion because it acts as thermal insulation and can isolate the effects of heat to more superficial tissues closer to the heat source.
Drug delivery and aerosols. Heated aerosol generation, airway modelling, and temperature-dependent deposition present more complex modelling requirements due to aerosol generation and propagation mechanics and shear-induced recombination and separation of aerosols. These affect aerosol size metrics, which then couple to mass transport dynamics. Phase change is also important, especially with hydrophilic aerosols. Bioheat enters where these phenomena affect tissue: a heated aerosol that impacts the throat, for example, brings thermal energy through deposition, creating a risk that must be assessed.
A Tiered Approach to Bioheat Modelling
Bioheat models are increasingly embedded in model-informed engineering decisions, providing concrete benefits across the product development cycle: early feasibility for bounding thermal risk, design iteration for optimizing geometry and power, verification to support test reduction, and submission evidence with risk-informed credibility assessments including targeted benchtop experimental validation.
As modelling becomes more central, the question is how to use it well. For bioheat in particular, a hierarchy-approach considers accuracy without going for the most complex models first:
- Baseline – Pennes with constant perfusion and conservative boundary conditions
- Enhanced – Pennes with temperature-dependent perfusion and damage models (Arrhenius or CEM43)
- Targeted Complexity – Explicit vessels and multiscale models (if inclusion is clinically relevant or justified)
All of these are decisions for the analyst to make, while weighing the trade-offs of effort against meaningful gains in accuracy for the decision at hand. ASME V&V 40 and the credibility assessments provided by it allow for these decisions to be justified for regulatory submissions.
Summary
Bioheat modelling has been refined from a simple extension of Fourier conduction to a complex, multiscale discipline. As is often the case in medical device development, complexity alone doesn’t determine success: the right level of physics for the decision at hand wins the day. The Pennes equation continues to be central because of its utility. Though not perfect, its track record reveals where assumptions hold and where shortfalls emerge, and modern approaches build on and refine it, occasionally replacing parts of it, but rarely discarding it entirely.
In computational modelling, the right balance of fidelity, practicality, and validation is what brings success in medical device design and development, resulting in safe and effective devices for patients.
Nathan Muller is a former StarFish Medical Mechanical Engineer – Analysis and Design. His focus is in simulation engineering using computational modelling. As part of a design and development team, he frequently leads the development of mechanical design and device integration across disciplines, including targeted optimization and derisking activities through computational modelling and simulation (CM&S).
Images: Adobe Stock
Related Resources
This article traces the Pennes bioheat equation from its 1948 origins to modern multiscale approaches, explaining how engineers select the right level of modelling complexity across device categories.

Five methods for building accurate project estimates, from gut feel to bottom-up, plus three add-ons that sharpen any estimate.

Designers and engineers today have no shortage of tools to improve designs, accelerate timelines, and meet cost targets. The challenge is knowing what to use and when.
Nick and Nigel breaks down what actually goes into the cost of getting a sterilized device into a user’s hands, and why up to 30% of costs can sit in places most teams don’t plan for.